
Abstract
Objective
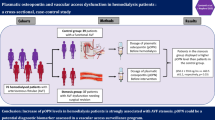
The aim of this study was to deduce the influence of atherosclerosis and plasma D-dimer concentration on the functioning of arteriovenous fistulae for hemodialysis.
Methods
The study was organized as a prospective and non-randomized investigation in the “Kragujevac” Clinical Center. The 81 examined patients, 49 (60.5%) males and 32 (39.5%) females, were divided into a group (n = 36) requiring several attempts to create arteriovenous fistulae for hemodialysis and a group (n = 45) with no complications of arteriovenous fistulae for hemodialysis. The demographic structure, etiology of renal disease, biochemical parameters and concentration of D-dimer were analyzed at the beginning of the study and 1 year later, as well as the existence of tissue calcification and Duplex ultrasound parameters of the carotid artery.
Results
The patients with arteriovenous fistulae complications were significantly older (58.4 ± 12.9 vs. 52.3 ± 11.6 years; P = 0.026). High venous pressure (98.6 ± 29.98 vs. 80 ± 33.57 mmHg; P = 0.005) and soft-tissue calcification (P = 0.03) were correlated with the occurrence of arteriovenous fistula complications. The greatest risk for failure of fistula was within the first month after creation of the anastomosis (failure rate was 0.235). The hemoglobin concentration (89 ± 14.0 vs. 96.6 ± 17.7 g/l; P = 0.048) was lower, and concentration of D-dimer at the end of the study was higher (219.56 ± 193.05 vs. 332.03 ± 149.48; P = 0.012) in patients with vascular access complications. By Cox regression analysis, the concentration of fibrin D-dimer at the end of the study was shown to be a significant predictor of fistula survival (β = 0.002; P = 0.006).
Conclusions
Complications of arteriovenous fistulae were more often recorded in older patients. The greatest risk for fistula functioning was within the first month after creation of the anastomosis. Vein pressure and anemia were important indicators of arteriovenous fistula complications. D-dimer was a significant marker of arteriovenous fistula thrombosis.

Similar content being viewed by others

Reference
Noon GP, Short D (1984) Dialysis access surgery. In: Suki WN, Massry SG (eds) Therapy of renal disease and related disorders, Martinus, Nijhoff Publishing, Dordrecht, pp 541–546
Kaneda H, Kaneda F, Shimoyamada K, Sakai S, Takahashi M (2003) Repeated femoral vein puncturing for maintenance hemodialysis vascular access. Nephrol Dial Transplant 18:1631–1638
Turmel-Rodrigues L, Mouton A, Birmele B et al (2001) Salvage of immature forearm fistulas for hemodialysis by interventional radiology. Nephrol Dial Transplant 16:2365–2371
Konner K, Nonnast-Daniel B, Ritz E (2003) Disease of the month. The arteriovenous fistula. J Am Soc Nephrol 14:1669–1680
Mercier E, Brange B, Vecina F et al (2001) Tissue factor coagulation pathway and blood cells activation state in renal insufficiency. Hematol J 2:18–25
Stenvinkel P, Pecoits-Filho R, Lindholm B (2003) Coronary artery disease in end-stage renal disease: no longer a simple plumbing problem. J Am Soc Nephrol 14:1927–1939
Umemura A, Yamada K (2001) B-Mode flow imaging of the carotid artery. Stroke 32:2055–2057
Handa N, Matsumoto M, Maeda H, Hougaku H, Kamada T (1995) For the OSACA study group. Ischemic stroke events and carotid atherosclerosis results of the Osaka follow-up study for ultrasonographic assessment of carotid atherosclerosis (the OSACA Study). Stroke 26:1781–1786
Papagianni A, Kalovoulos M, Kirmizis D et al (2003) Carotid atherosclerosis is associated with inflammation and endothelial cell adhesion molecules in chronic hemodialysis patients. Nephrol Dial Transplant 18:113–119
Rodrigez JA, Armadanas L, Ferrer E et al (2000) The function permanent vascular access. Nephrol Dial Transplant 15:402–408
Robbin ML, Chamberlain NE, Lockhart ME et al (2002) Hemodialysis arteriovenous fistula maturity: US evaluation. Radiology 225:259
Guera A, Raynaud A, Beyssen B et al (2002) Arterial percutaneus angioplasty in upper limbs with vascular access devices for hemodialysis. Nephrol Dial Transplant 17:843–851
Fujisawa M, Haramaki R, Miyazaki H, Imaizumi T, Okuda S (2000) Role of lipoprotein(a) and TGF-ß1 in atherosclerosis of hemodialysis patients. J Am Soc Nephrol 11:1889–1895
Fabbian F, Catalano C, Orlandi V, Conte MM, Lupo A, Catizone L (2005) Evaluation of aortic arch calcification in hemodialysis patients. J Nephrol 18:289–293
Lindsay RM, Alhejaili F, Nesrallah G et al (2003) Calcium and phosphate balance with quotidian hemodialysis. Am J Kidney Dis 42:24–29
Saran R, Dykstra DM, Pisoni RL et al (2004) Timing of first cannulation and vascular access failure in hemodialysis: an analysis of practice patterns at dialysis facilities in the DOPPS. Nephrol Dial Transplant 19:2334–2340
Turmel-Rodrigues LA (2000) Hemodialysis access declotting: a native fistula is not a prosthetic graft. J Vasc Interven Radiol 11:135–137
Segarra A, Chacon P, Martinez-Eyarre C et al (2001) Circulating levels of plasminogen activator inhibitor type-1, tissue plasminogen activator and thrombomodulin in hemodialysis patients: biochemical correlations and role as independent predictors of coronary artery stenosis. J Am Soc Nephrol 12:1255–1263
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stolic, R.V., Trajkovic, G.Z., Peric, V.M. et al. The influence of atherosclerosis and plasma D-dimer concentration in patients with a functioning arteriovenous fistula for maintenance hemodialysis. Int Urol Nephrol 40, 503–508 (2008). https://doi.org/10.1007/s11255-007-9321-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-007-9321-8